 |
Mechanisms of Myopia: What We Know & What We Wonder
With an increase in prevalence and severity, there is a growing interest in the pathophysiology of this condition.
By Erin S. Tomiyama, OD, PhD
Release Date: January 15, 2023
Expiration Date: January 15, 2026
Estimated Time to Complete Activity: 2 hours
Jointly provided by Postgraduate Institute for Medicine (PIM) and Review Education Group
Educational Objectives: After completing this activity, the participant should be better able to:
Recognize the pathophysiology and mechanisms of myopia.
Explain the role genetics plays in the development and progression of this condition.
Identify the environmental factors that contribute to myopia.
Educate patients and their parents on what they can do.
Target Audience: This activity is intended for optometrists engaged in myopia management.
Accreditation Statement: In support of improving patient care, this activity has been planned and implemented by PIM and the Review Education Group. PIM is jointly accredited by the Accreditation Council for Continuing Medical Education, the Accreditation Council for Pharmacy Education and the American Nurses Credentialing Center to provide CE for the healthcare team. PIM is accredited by COPE to provide CE to optometrists.
Reviewed by: Salus University, Elkins Park, PA
Faculty/Editorial Board: Erin S. Tomiyama, OD, PhD
Credit Statement: This course is COPE approved for 2 hours of CE credit. Activity #125288 and course ID 82547-GO. Check with your local state licensing board to see if this counts toward your CE requirement for relicensure.
Disclosure Statements: PIM requires faculty, planners and others in control of educational content to disclose all their financial relationships with ineligible companies. All identified conflicts of interest are thoroughly vetted and mitigated according to PIM policy. PIM is committed to providing its learners with high-quality, accredited CE activities and related materials that promote improvements or quality in healthcare and not a specific proprietary business interest of an ineligible company.
Those involved reported the following relevant financial relationships with ineligible entities related to the educational content of this CE activity: Author: Dr. Tomiyama receives consulting fees from Vyluma and conducts research with CooperVision. Managers and Editorial Staff: The PIM planners and managers have nothing to disclose. The Review Education Group planners, managers and editorial staff have nothing to disclose.
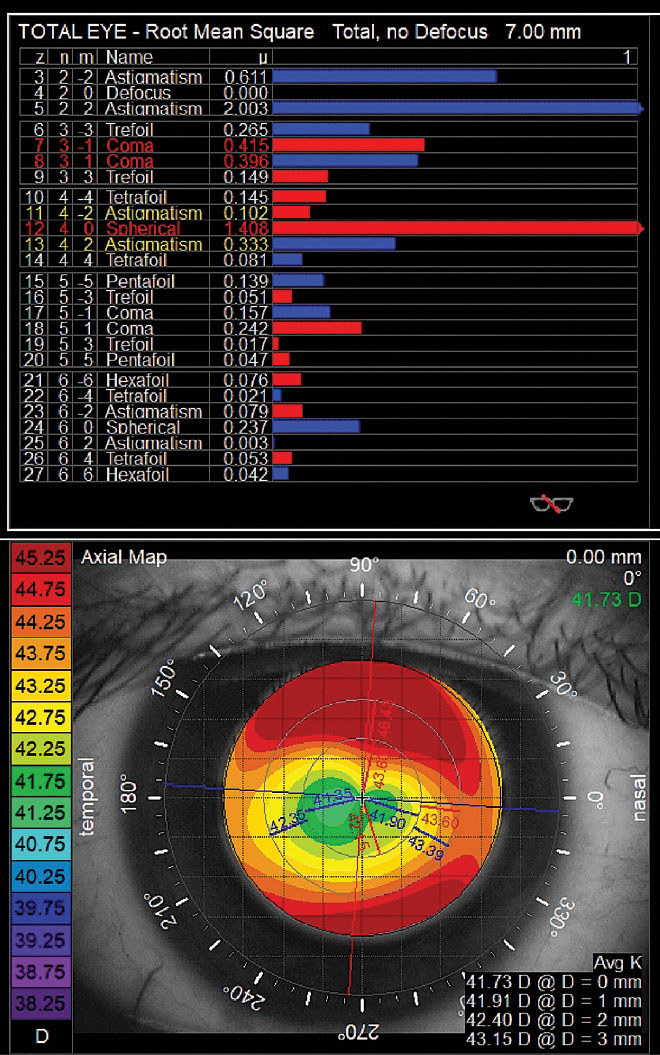 |
| Higher-order aberrations measured after orthokeratology lens wear. Primary coma and spherical aberration are elevated to outside normal limits. Corneal topography shows central flattening with an incomplete treatment ring. Click image to enlarge. |
Myopia is a result of a mismatch between the refractive power of the eye and its axial length, most commonly from the eye growing too long.1 In the United States, the prevalence of myopia increased from 25% in 1971 to 1972 to 42% in 1999 to 2004, and worldwide, the condition’s prevalence is expected to reach 50% by 2050.2,3 With an increase in prevalence and severity, the interest in the pathophysiology and mechanisms of myopia follows. Treatments such as atropine, orthokeratology and peripheral defocus contact lenses are used to slow the progression of myopia after it develops, but a better understanding of the causes of myopia could delay or prevent onset altogether.4-9
While there has been an exponential increase in myopia literature over the last few decades, the main focus has been on slowing myopia progression. And so, there are still several unknowns regarding the pathophysiology of this condition and the roles both genetics and the environment play in myopia development and progression. In this article, we will delve deeper into the mechanisms of myopia and explore several key areas that require further investigation as to how they might impact optometric practices.
Role of HOAs in Myopia Development
Higher-order aberrations (HOAs) can degrade retinal image quality and may interact with lower-order aberrations to change the optics of the eye. These changes may play a role in refractive development and the emmetropization process.10 Some studies suggest an increase in HOAs, specifically spherical aberration and coma, is associated with myopia, while others suggest there is no change in HOAs with myopia.11-15
Mixed results have also been observed in longitudinal studies evaluating the relationship between HOAs and axial elongation. However, age, degree of myopia and method of measurement were confounding variables.16-18 More recently, one study found that increased levels of HOAs were associated with slower axial elongation.19 This is perhaps due to the HOAs altering the retinal image quality and serving as a directional cue to slow eye growth. Further longitudinal studies are needed to fully understand the role of HOAs in the emmetropization process.
There is strong evidence to support the notion that current optical treatments for myopia management also induce more HOAs.20 This increase in HOAs could play a part in how these optical devices, specifically orthokeratology and multifocal soft lenses, slow myopia progression.
Pathophysiology Differences Between Myopia Types
Most forms of myopia occur because the axial length is too long relative to the refractive power of the eye, otherwise known as axial myopia.21 Conversely, there are conditions, such as keratoconus, where myopia results from corneal changes rather than axial elongation.22 There are several hundred genetic conditions that feature myopia and involve various molecular pathways, but these rare conditions only account for less than 1% of the myopic population.23 The most common form of myopia—school-age myopia—is impacted by both the environment and gene expression.21 However, adult-onset myopia may have a different pathophysiology given that it develops later in life. Adult-onset myopia is commonly associated with near work and usually limited to low or moderate levels.24 Therefore, the degree to which genetics play a role in myopia development may vary by type, but school-age myopia has been found to have both genetic and environmental components.
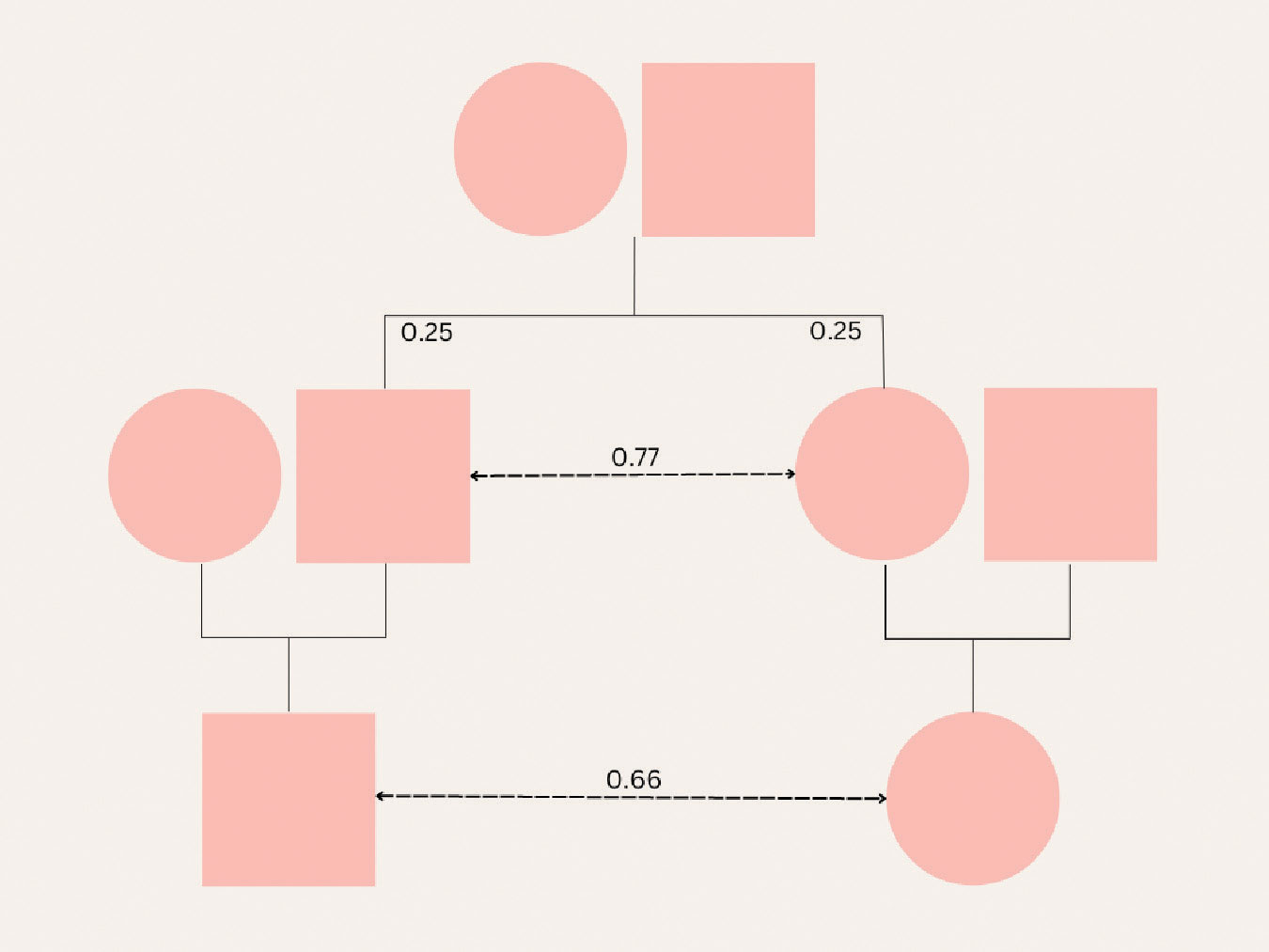 |
A family tree shows the lowest heritability of myopia exists between parent and daughter/son. There is a greater heritability between siblings and cousins, which points to an environmental rather than a genetic cause. Click image to enlarge. |
Disease Development and Genetics
There is an ongoing debate as to whether nature or nurture prevails in the development of myopia. Initial thoughts of a genetic basis for myopia come from a greater relationship of refractive error in monozygotic compared with dizygotic twins.25 Overall, several twin studies continued to demonstrate high heritability, but this could be confounded with shared environmental factors such as location and education. However, one twin study investigated refractive error development in twin pairs reared separately and found greater similarity among monozygotic twins compared with dizygotic, indicating a genetic influence.26
Parental myopia is a risk factor for child myopia. One myopic parent increases the risk by threefold and two myopic parents by sixfold.27 While genetics could be the primary driver of this increased risk, there are also other factors at play, such as lifestyle and upbringing. Further studies showed that there was a greater correlation between refractive errors of siblings than of children and their parents, implying that environment has a predominant role. Even correlations between cousins were almost as high as between siblings, highlighting contemporary environmental factors.28
Genome-wide association studies compare genetic information across large groups of people to identify single nucleotide polymorphisms that are associated with a particular trait. The combined efforts of 23andMe and the Consortium for Refractive Error and Myopia (CREAM) have identified 161 potential gene loci involved in myopia.29 These studies have advanced our understanding of genetic mapping and potential loci associated with myopia, but ultimately these genetic variations only account for about 8% of the variation in refractive error.30
Other evidence to support a strong genetic component is the variation in the prevalence of myopia between different racial and ethnic groups. However, there can be large genetic variation between, and even within, populations.31 Differences between populations are usually a result of rare alleles that would more readily disappear due to genetic drift, so it is unlikely this contributes to the high prevalence of myopia we see today.32 Additionally, this genetic variation could also be confounded by location and environment.
While it is clear that there is a genetic component to myopia development, genetics cannot single-handedly be responsible for the dramatic rise in the condition.21 The lack of causal evidence from specific genes and the fact that it is a locally regulated process both support this argument. Myopia is a multifactorial disease that also has an environmental component.
 |
Outdoor environments provide higher light intensity, varying spectral composition of light and flatter dioptric demands, all of which may contribute to delayed myopia onset. Click image to enlarge. |
Impact of Environmental Factors
Emmetropization is a local, visually regulated process, thereby suggesting that myopia development is also modulated by visual signals perceived by the retina.33 Several potential environmental elements could contribute, but study limitations and confounding factors prevent us from fully understanding these factors.1 The two prevailing environmental factors are near work and outdoor time, which are discussed in more detail later.
Additional environmental and behavioral factors that have been explored include intelligence, physical activity, socioeconomic status and lived environment (rural vs. urban).34 It could be hypothesized that intelligence is a surrogate for education or near work and physical activity for outdoor time. It has long been reported that members of higher socioeconomic status are more likely to develop myopia, but this could be associated with family income, parental myopia, parental education or near work demands.35 It is unlikely that socioeconomic status itself is the direct cause of myopia, but perhaps it serves as a covariate for education and near work.34
Related to all these environmental factors is difference in lived environment. A greater prevalence of myopia has been found in more urban environments, but this could be related to education and outdoor time.36 Those of higher socioeconomic status may live in more urban environments with greater population densities.37 Urban environments also tend to have less access to green space, which could be a proxy for outdoor time.38 In considering differences in the amount of outdoor time in urban vs. rural settings, other factors could include safety, weather, pollution and cultural attitudes.34
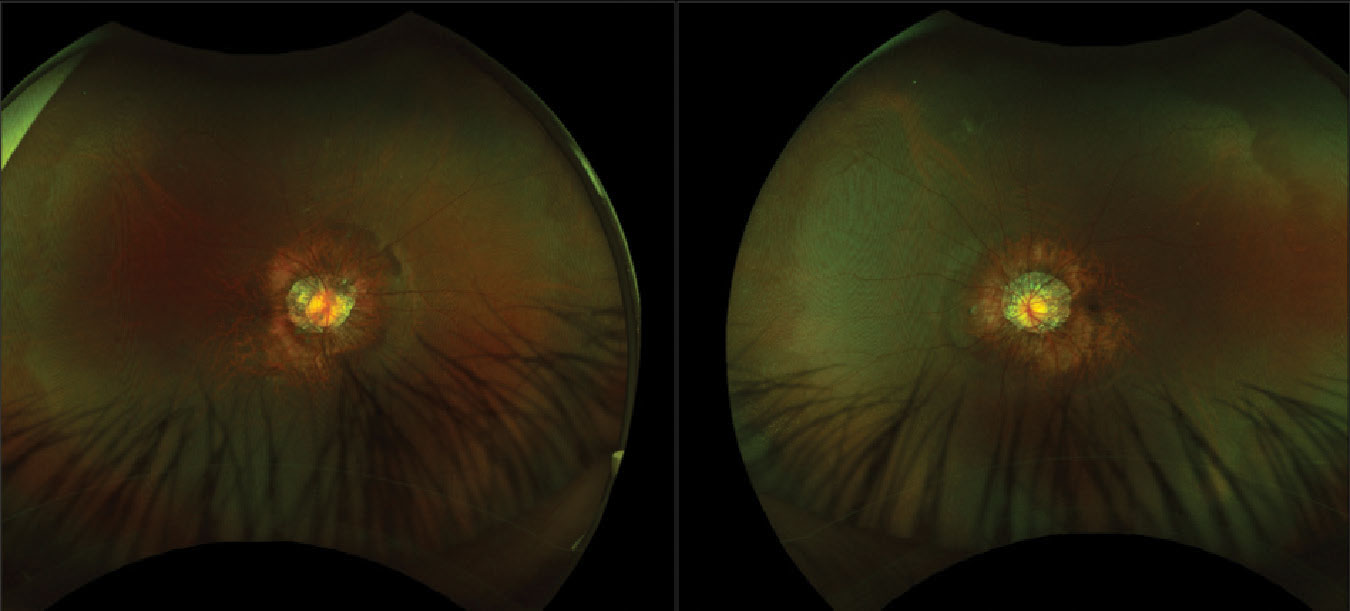 |
Fundus photos of the right and left eyes show posterior staphylomas, common among high myopes, with peripapillary atrophy around the optic nerve heads. White without pressure can be seen in the periphery of both eyes. Click image to enlarge. |
Education and Associated Near Work
The theory that myopia is related to education is based on the finding that the prevalence of myopia is higher in areas where there is an emphasis on education and more children complete more years of schooling.23 Similarly, children who achieve higher grades and adults who complete higher educational levels tend to be more myopic.27,39 The relationship between myopia and educational level is wrapped up in the confounding factors of ethnicity and increased near work.
It has been thought that there are academic pressures and more intense schooling undertaken by East Asian populations that could contribute to the higher prevalence of myopia among this group.40 One study explored near work differences among East Asian and Caucasian groups and found that East Asian participants reported longer periods of near work, specifically with homework and computer use, that could be related to academic demands (differences in schools and participation in after-school programs, such as tutoring).41 A meta-analysis found that there was a larger genetic influence on Asian participants with higher vs. lower levels of education but no significant interaction with European participants.42 Additionally, a Mendelian randomization study showed that there is a causal relationship between educational attainment and refractive error.43 It is clear that ethnicity is a risk factor for myopia development but also possible that differences in near work behavior and genetics among different ethnic groups augment this risk.
While there is a relationship between myopia and near work, it is potentially the intensity rather than the total duration of near work that is the primary driver.41 Both closer working distances and longer time spent doing continuous reading were associated with a greater risk of myopia.41
Accommodation was also thought to play a role in near work, as near targets require a higher accommodative demand, which leads to increased accommodative lag that causes hyperopic defocus on the retina, stimulating axial elongation. Studies evaluating accommodative lag have shown that the increase in lag or under-accommodation occurs after the onset of myopia and is likely not causal.44 Support for this accommodation theory grew when atropine, a topical agent that blocks accommodation, was shown to prevent myopia development. However, animal studies with chicks showed that atropine prevents myopia even though their accommodative system is mediated by nicotinic receptors; therefore, accommodation was shown to have no role in myopia onset or progression.45,46
 |
| With myopia on the rise, practitioners must implement myopia management therapies and recommend behavioral modifications to lower the risk of high myopia in the future. Click image to enlarge. |
Relationship Between Digital Screen Time and Myopia
In today’s world, the type of near work has changed to increased use of computers, digital devices, video games and virtual reality. While parents are quick to blame excessive screen time for their child’s myopia, the prevalence of the condition was increasing before the widespread use of digital devices.47 However, with advances in technology and increasing use in schools, children are becoming digital users at a younger age. The World Health Organization points out that screen time may promote sedentary behavior that negatively impacts overall health, and some countries have imposed limitations of screen time in children.48
A systematic review of 15 studies included 11 on myopia prevalence and four on myopia progression.47 Six of the 11 studies revealed a relationship between computer use and the prevalence of myopia, while the other five did not. The pooled odds ratio suggests there is no relationship between screen time and myopia, though there are some confounding variables such as education intensity, time spent on schoolwork/homework, recall bias and near work. It is also likely that screen time is a substitution for paper and pen reading/writing, not outdoor time.47
The COVID-19 lockdown provided a unique opportunity to study the effects of home confinement on myopia. During this period, there was less outdoor time, more indoor time, more screen time and more near work.49 One study evaluated over 120,00 children in China who underwent noncycloplegic photorefraction.50 The team found a myopic shift of -0.30D and an increase in myopia prevalence among six- to eight-year-olds compared with the years leading up to the epidemic (2015 to 2019); however, it is important to note that the measurements were noncycloplegic and taken with a photoscreener device.50
Understanding the Role of Outdoor Time
While this is one of the main modifiable risk factors for myopia development, the specific components of outdoor time remain unknown.
Protecting against myopia. Parents often ask how much time outdoors is needed. The Sydney Myopia Study showed that exposure of at least two hours per day was associated with a decreased risk of myopia development.51 In 2012, a meta-analysis revealed that each additional hour spent outdoors per week reduced the odds of myopia by 2%.52
It is clear there is a dose-dependent response between increased time outdoors and the risk of myopia onset. One study found that an increase of 76 minutes per day is needed to reduce the incidence of myopia by 50%.53 The main limitation to all of these studies is recall bias from the use of questionnaires where patients/parents report the amount of time spent outdoors. More recently, the development of wearable technology has allowed for more objective measures of outdoor time, such as light exposure and activity.54,55 However, wearable devices are still subject to proper use (i.e., remembering to wear and charge the device), and the location of the device on the body may not be truly representative of the visual input.
In addition to the total time spent outdoors, taking an outdoor break directly after prolonged near work may be more effective. Researchers showed that, in chicks, a brief period of bright light exposure, simulating outdoor time, after minus defocus can help negate the signals for developing myopia.56 Animal research has also shown that there may be a role in the timing and intervals of bright light exposure, rather than the cumulative daily exposure, that could disrupt normal circadian rhythm.57
Ultimately, a recommendation of two hours per day of outdoor time should be made to pre-myopic children. Specifics as to the timing or intervals of time outdoors will be elucidated with further research.
Delaying disease onset. There are several proposed reasons why increased outdoor time is linked with a lower incidence of myopia: higher light intensity, spectral composition of light and dioptric demand. Outdoor ambient illumination varies from 1,000 to 150,000 lux.55 Rearing animals in a high-light environment has a protective effect against form-deprivation myopia but less so against lens-induced myopia.58,59
The primary theory behind high-light intensity is that brighter light triggers increased dopamine release from the retina, which slows axial elongation.60-62 Dopamine also modulates retinal circadian rhythm, and other diurnal rhythms have been found in components of eye growth (i.e., axial length and choroidal thickness).57 It is possible that both light-regulated dopamine release and/or disruptions of circadian pathways could be involved in axial elongation.34 Melatonin is another modulator of circadian rhythm with a reciprocal relationship to dopamine. Myopes have been shown to have higher levels of melatonin in the morning and poorer sleep quality.63 Light exposure can promote dopamine release and suppress melatonin, both involved in modulating circadian rhythm, which may be required for the emmetropization process.
Another possible theory of high-light intensity is that increased ultraviolet light stimulates the production of vitamin D, which protects against myopia development. Though it has been shown that myopes have lower levels of vitamin D, there is no evidence of a causal relationship.64,65
The spectral composition of light varies between indoor and outdoor environments, time of day and season.66 Longitudinal chromatic aberrations cause different wavelengths of light to come into focus at different positions. Short blue wavelengths come into focus in front of long red wavelengths. Rearing animals in monochromatic conditions results in a disruption of the emmetropization process. Conflicting results are presented, where long-wavelength red light causes myopia in chicks and guinea pigs but hyperopia in tree shrews and monkeys.67-70 The exact opposite was found with chicks, guinea pigs and tree shrews in relation to short-wavelength blue light.
In the last year, several studies have looked at the use of low-intensity red light therapy as a treatment for myopia management in children in East Asia. Most used a protocol of three minutes, twice per day, of 635nm to 650nm red light administered via desktop light with at least four hours between each session.71-75 The studies are all in agreement that children who are treated with low-intensity red light have less spherical equivalent refractive error changes and less axial elongation than children not receiving treatment. There are conflicting results regarding choroidal thickness changes, but most found an increase in choroidal thickness after red light therapy.71,76,77 The one study that did not compared two eyes within a participant, with only one eye receiving red light treatment.78 Though most data are presented for 12 months or less, two studies have already evaluated efficacy after treatment cessation and shown there is a moderate rebound effect.76,79 Though promising, the use of low-intensity red light therapy is not approved in the United States, as there are insufficient data on its long-term safety. More longitudinal data are needed to fully understand the risks and benefits of low-intensity red light therapy.
While the focus has been on long-wavelength red light, one study evaluated the use of short-wavelength blue light and found that it decreased axial length with no significant change in choroidal thickness.80 Participants were exposed to blue light for one hour, and hyperopic defocus was induced by a minus lens over one eye. The change in axial length was small (less than 10µm), so more studies are needed to show the efficacy of short-wavelength blue light.
Lastly, the dioptric demand of an outdoor environment is often much flatter than an indoor setting. Near stimuli in an indoor environment cause hyperopic defocus on the retina.81 A recent study evaluated over 800 images of different indoor and outdoor settings and found that man-made outdoor and indoor environments lacked high spatial frequencies and created spatial frequency profiles that were similar to Bangerter filters used to induce form deprivation myopia in animals.82
Preventing disease progression. A summary of four randomized controlled trials done in East Asia shows that increased outdoor time reduces myopia incidence by 5% to 10% but has little effect on slowing progression.1,83-86 The reported reduction in myopia progression in myopic participants was 0.17D to 0.23D with a 0.03mm to 0.15mm reduction in axial elongation over the one- to three-year study period. A meta-analysis of 25 studies confirmed that there is a protective effect of increased outdoor time in delaying myopia onset of non-myopic children, but no effect on myopia progression of children who are already myopic was noted.53 However, there is evidence that the rate of myopia progression can be regulated by environmental factors. Specifically, there are seasonal differences in myopia progression showing slower rates in summer than in winter.87,88 A few studies have reported that more outdoor time does indeed slow myopia progression.89,90
Myopic children spend less time outdoors compared with non-myopic children.91,92 While the evidence may be inconclusive, increased outdoor time is still an important public health recommendation for children that aligns with initiatives to promote a healthier lifestyle.93 Additionally, delaying the onset of myopia will slow myopia progression since it is largely age-dependent and will also decrease the level of final myopia.93
Navigating the Unknown
Despite several advances in the understanding of myopia development and progression, there are still many unknowns. It is imperative that practitioners continue to stay on top of education in this area so they can practice evidence-based optometry. As this public health issue continues to grow, optometrists should aim to first delay or prevent the onset of myopia. By delaying onset, we can reduce the severity of an individual’s myopia and decrease the prevalence of high myopia and the risk of ocular consequences that follow. Practitioners can educate parents and patients about myopia development and recommend behavioral modifications such as increased outdoor time and decreased near work, with breaks and increased working distances. Once children develop myopia, treatments alone or in combination should be implemented to slow the progression.
To answer the age-old question of nature vs. nurture, there are aspects of both genetics and environment that play a role in myopia development. The increase in myopia prevalence has dramatically exceeded the increase that would be expected from genetic variability. So, while there may be genetic susceptibility, it cannot be the only cause of myopia. There is resounding evidence that environmental factors influence the development of myopia. With environmental modifications, there is hope that we can win the battle against myopia.
Dr. Tomiyama is an assistant professor of optometry at Marshall B. Ketchum University, where she offers a contact lens curriculum and serves as a clinical attending in the Stein Family Cornea & Contact Lens Center. She recently established the Myopia Management Service at the university. She receives consulting fees from Vyluma and conducts research with CooperVision.
1. Harb EN, Wildsoet CF. Origins of refractive errors: environmental and genetic factors. Annu Rev Vis Sci. 2019;5(1):47-72. 2. Vitale S. The refractive status and vision profile A questionnaire to measure vision-related quality of life in persons with refractive error. Ophthalmology. 2000;107(8):1529-39. 3. Holden BA, Fricke TR, Wilson DA, et al. Global prevalence of myopia and high myopia and temporal trends from 2000 through 2050. Ophthalmology. 2016;123(5):1036-42. 4. Chua WH, Balakrishnan V, Chan YH, et al. Atropine for the treatment of childhood myopia. Ophthalmology. 2006;113(12):2285-91. 5. Yam JC, Jiang Y, Tang SM, et al. Low-concentration atropine for myopia progression (LAMP) study. Ophthalmology. 2019;126(1):113-24. 6. Cho P, Cheung SW. Retardation of myopia in orthokeratology (ROMIO) study: A 2-year randomized clinical trial. Invest Opthalmol Vis Sci. 2012;53(11):7077. 7. Cho P, Cheung SW, Edwards M. The longitudinal orthokeratology research in children (LORIC) in Hong Kong: A pilot study on refractive changes and myopic control. Curr Eye Res. 2005;30(1):71-80. 8. Walline JJ, Walker MK, Mutti DO, et al. Effect of high add power, medium add power, or single-vision contact lenses on myopia progression in children. JAMA. 2020;324(6):571-80. 9. Chamberlain P, Peixoto-de-Matos SC, Logan NS, et al. A 3-year randomized clinical trial of MiSight lenses for myopia control. Optom Vis Sci. 2019;96(8):556-67. 10. Chakraborty R, Ostrin LA, Benavente-Perez A, et al. Optical mechanisms regulating emmetropisation and refractive errors: evidence from animal models. Clin Exp Optom. 2020;103(1):55-67. 11. He JC, Sun P, Held R, et al. Wavefront aberrations in eyes of emmetropic and moderately myopic school children and young adults. Vision Res. 2002;42(8):1063-70. 12. Paquin MP, Hamam H, Simonet P. Objective measurement of optical aberrations in myopic eyes. Optom Vis Sci. 2002;79(5):285-91. 13. Carkeet A, Dong Luo H, Tong L, et al. Refractive error and monochromatic aberrations in Singaporean children. Vision Res. 2002;42(14):1809-24. 14. Atchison DA, Schmid KL, Pritchard N. Neural and optical limits to visual performance in myopia. Vision Res. 2006;46(21):3707-22. 15. Cheng X, Bradley A, Hong X, et al. Relationship between refractive error and monochromatic aberrations of the eye. Optom Vis Sci. 2003;80(1):43-9. 16. Philip K, Sankaridurg P, Holden B, et al. Influence of higher order aberrations and retinal image quality in myopisation of emmetropic eyes. Vision Res. 2014;105:233-43. 17. Zhang N, Yang XB, Zhang WQ, et al. Relationship between higher-order aberrations and myopia progression in schoolchildren: A retrospective study. Int J Ophthalmol. 2013;6(3):295-99. 18. Hiraoka T, Kotsuka J, Kakita T, et al. Relationship between higher-order wavefront aberrations and natural progression of myopia in schoolchildren. Sci Rep. 2017;7(1):7876. 19. Lau JK, Vincent SJ, Collins MJ, et al. Ocular higher-order aberrations and axial eye growth in young Hong Kong children. Sci Rep. 2018;8(1):2-11. 20. Tomiyama ES, Hu C, Marsack JD, et al. Greater higher order aberrations induced by toric orthokeratology versus soft toric multifocal contact lens wear. Ophthalmic Physiol Opt. 2021;41(4):726-35. 21. Morgan IG, Rose KA. Myopia: is the nature-nurture debate finally over? Clin Exp Optom. 2019;102(1):3-17. 22. Gordon-Shaag A, Millodot M, Shneor E, et al. The genetic and environmental factors for keratoconus. Biomed Res Int. 2015;2015:1-19. 23. Morgan IG, French AN, Ashby RS, et al. The epidemics of myopia: Aetiology and prevention. Prog Retin Eye Res. 2018;62:134-49. 24. Bullimore MA, Reuter KS, Jones LA, et al. The study of progression of adult nearsightedness (SPAN): Design and baseline characteristics. Optom Vis Sci. 2006;83(8):594-604. 25. Sorsby A, Sheridan M, Leary G. Refraction and Its Components in Twins. Her Majesty’s Stationery Office; 1962. 26. Knobloch W, Leavenworth N, Bouchard T, et al. Eye findings in twins reared apart. Ophthalmic Paediatric Genetics. 1985;5:59-66. 27. Mutti DO, Mitchell GL, Moeschberger ML, et al. Parental myopia, near work, school achievement, and children’s refractive error. Invest Ophthalmol Vis Sci. 2002;43(12):3633-40. 28. Chen CYC, Scurrah KJ, Stankovich J, et al. Heritability and shared environment estimates for myopia and associated ocular biometric traits: the Genes in Myopia (GEM) family study. Hum Genet. 2007;121(3-4):511-20. 29. Tedja MS, Wojciechowski R, Hysi PG, et al. Genome-wide association meta-analysis highlights light-induced signaling as a driver for refractive error. Nat Genet. 2018;50(6):834-48. 30. Verhoeven VJM, Hysi PG, Wojciechowski R, et al. Genome-wide meta-analyses of multiancestry cohorts identify multiple new susceptibility loci for refractive error and myopia. Nat Genet. 2013;45(3):314-8. 31. Risch N. Dissecting racial and ethnic differences. N Engl J Med. 2006;354(4):408-11. 32. Auton A, Abecasis GR, Altshuler DM, et al. A global reference for human genetic variation. Nature. 2015;526(7571):68-74. 33. Smith EL, Hung LF, Arumugam B. Visual regulation of refractive development: insights from animal studies. Eye. 2014;28(2):180-8. 34. Morgan IG, Wu PC, Ostrin LA, et al. IMI risk factors for myopia. Invest Ophthalmol Vis Sci. 2021;62(5):12-5. 35. Ware J. Observations relative to the near and distant sight of different persons. Philos Trans R Soc Lond. 1813;103:31-50. 36. Ip JM, Rose KA, Morgan IG, et al. Myopia and the urban environment: Findings in a sample of 12-year-old Australian school children. Invest Ophthalmol Vis Sci. 2008;49(9):3858. 37. Morris TT, Guggenheim JA, Northstone K, et al. Geographical variation in likely myopia and environmental risk factors: A multilevel cross classified analysis of a UK cohort. Ophthalmic Epidemiol. 2020;27(1):1-9. 38. Dadvand P, Sunyer J, Alvarez-Pedrerol M, et al. Green spaces and spectacles use in schoolchildren in Barcelona. Environ Res. 2017;152:256-62. 39. Mountjoy E, Davies NM, Plotnikov D, et al. Education and myopia: assessing the direction of causality by mendelian randomisation. BMJ. 2018;361:k2022. 40. Ip JM, Huynh SC, Robaei D, et al. Ethnic differences in refraction and ocular biometry in a population-based sample of 11-15-year-old Australian children. Eye. 2008;22(5):649-56. 41. Ip JM, Saw SM, Rose KA, et al. Role of near work in myopia: Findings in a sample of Australian school children. Invest Ophthalmol Vis Sci. 2008;49(7):2903. 42. Fan Q, Verhoeven VJM, Wojciechowski R, et al. Meta-analysis of gene-environment-wide association scans accounting for education level identifies additional loci for refractive error. Nat Commun. 2016;7. 43. Cuellar P, Lu Y, Kho PF, et al. Assessing the genetic predisposition of education on myopia: A Mendelian randomization study. 2014;67(3):223-30. 44. Mutti DO, Mitchell GL, Hayes JR, et al. Accommodative lag before and after the onset of Myopia. Invest Ophthalmol Vis Sci. 2006;47(3):837. 45. McBrien NA, Moghaddam HO, Reeder AP. Atropine reduces experimental myopia and eye enlargement via a nonaccommodative mechanism. Invest Ophthalmol Vis Sci. 1993;34(1):205-15. 46. Logan NS, Radhakrishnan H, Cruickshank FE, et al. IMI accommodation and binocular vision in myopia development and progression. Invest Ophthalmol Vis Sci. 2021;62(5):4. 47. Lanca C, Saw SM. The association between digital screen time and myopia: A systematic review. Ophthalmic Physiol Opt. 2020;40(2):216-29. 48. World Health Organization. WHO Guidelines on Physical Activity, Sedentary Behaviour and Sleep for Children under 5 Years of Age.; 2019. 49. Limwattanayingyong J, Amornpetchsathaporn A, Chainakul M, et al. The association between environmental and social factors and myopia: A review of evidence from COVID-19 pandemic. Front Public Health. 2022;10:918182 50. Wang J, Li Y, Musch DC, et al. Progression of myopia in school-aged children after COVID-19 home confinement. JAMA Ophthalmol. 2021;139(3):293-300. 51. Rose KA, Morgan IG, Ip J, et al. Outdoor activity reduces the prevalence of myopia in children. Ophthalmology. 2008;115(8):1279-85. 52. Sherwin JC, Reacher MH, Keogh RH, et al. The association between time spent outdoors and myopia in children and adolescents. Ophthalmology. 2012;119(10):2141-51. 53. Xiong S, Sankaridurg P, Naduvilath T, et al. Time spent in outdoor activities in relation to myopia prevention and control: a meta-analysis and systematic review. Acta Ophthalmol. 2017;95(6):551-66. 54. Read SA, Collins MJ, Vincent SJ. Light exposure and physical activity in myopic and emmetropic children. Optom Vis Sci. 2014;91(3):330-41. 55. Ostrin LA. Objectively measured light exposure in emmetropic and myopic adults. Optom Vis Sci. 2017;94(2):229-38. 56. Zhu X, Wallman J. Temporal properties of compensation for positive and negative spectacle lenses in chicks. Invest Ophthalmol Vis Sci. 2009;50(1):37-46. 57. Chakraborty R, Ostrin LA, Nickla DL, et al. Circadian rhythms, refractive development, and myopia. Ophthalmic Physiol Opt. 2018;38(3):217-45. 58. Smith EL, Hung LF, Huang J. Protective effects of high ambient lighting on the development of form-deprivation myopia in Rhesus monkeys. Invest Ophthalmol Vis Sci. 2012;53(1):421. 59. Smith EL, Hung LF, Arumugam B, et al. Negative lens-induced myopia in infant monkeys: effects of high ambient lighting. Invest Ophthalmol Vis Sci. 2013;54(4):2959. 60. Schaeffel F, Hagel G, Bartmann M, et al. 6-Hydroxy dopamine does not affect lens-induced refractive errors but suppresses deprivation myopia. Vision Res. 1994;34(2):143-9. 61. Li XX, Schaeffel F, Kohler K, et al. Dose-dependent effects of 6-hydroxy dopamine on deprivation myopia, electroretinograms, and dopaminergic amacrine cells in chickens. Vis Neurosci. 1992;9(5):483-92. 62. Bartmann M, Schaeffel F, Hagel G, et al. Constant light affects retinal dopamine levels and blocks deprivation myopia but not lens-induced refractive errors in chickens. Vis Neurosci. 1994;11(2):199-208. 63. Ostrin LA. Ocular and systemic melatonin and the influence of light exposure. Clin Exp Optom. 2019;102(2):99-108. 64. Yazar S, Hewitt AW, Black LJ, et al. Myopia is associated with lower vitamin D status in young adults. Invest Ophthalmol Vis Sci. 2014;55(7):4552. 65. Guggenheim JA, Williams C, Northstone K, et al. Does vitamin D mediate the protective effects of time outdoors on myopia? Findings from a prospective birth cohort. Invest Ophthalmol Vis Sci. 2014;55(12):8550-8. 66. Thorne HC, Jones KH, Peters SP, et al. Daily and seasonal variation in the spectral composition of light exposure in humans. Chronobiol Int. 2009;26(5):854-66. 67. Foulds WS, Barathi VA, Luu CD. Progressive myopia or hyperopia can be induced in chicks and reversed by manipulation of the chromaticity of ambient light. Invest Ophthalmol Vis Sci. 2013;54(13):8004. 68. Liu R, Qian YF, He JC, et al. Effects of different monochromatic lights on refractive development and eye growth in guinea pigs. Exp Eye Res. 2011;92(6):447-53. 69. Gawne TJ, Siegwart JT, Ward AH, et al. The wavelength composition and temporal modulation of ambient lighting strongly affect refractive development in young tree shrews. Exp Eye Res. 2017;155:75-84. 70. Smith EL, Hung LF, Arumugam B, et al. Effects of long-wavelength lighting on refractive development in infant Rhesus monkeys. Invest Ophthalmol Vis Sci. 2015;56(11):6490. 71. Zhou L, Xing C, Qiang W, et al. Low-intensity, long-wavelength red light slows the progression of myopia in children: an Eastern China-based cohort. Ophthalmic Physiol Opt. 2022;42(2):335-44. 72. Tian L, Cao K, Ma DL, et al. Investigation of the Efficacy and safety of 650 nm low-level red light for myopia control in children: A randomized controlled trial. Ophthalmol Ther. 2022;11(6):2259-70. 73. Chen Y, Xiong R, Chen X, et al. Efficacy comparison of repeated low-level red light and low-dose atropine for myopia control: A randomized controlled trial. Transl Vis Sci Technol. 2022;11(10):1-9. 74. Jiang Y, Zhu Z, Tan X, et al. Effect of repeated low-level red-light therapy for myopia control in children: A multicenter randomized controlled trial. Ophthalmology. 2022;129(5):509-19. 75. Dong J, Zhu Z, Xu H, et al. Myopia control effect of repeated low-level red-light therapy in Chinese children: A randomized, double-blind, controlled clinical trial. Ophthalmology. 2022;S0161-6420(22)00669-8. 76. Chen H, Wang W, Liao Y, et al. Low-intensity red-light therapy in slowing myopic progression and the rebound effect after its cessation in Chinese children: a randomized controlled trial. Graefes Arch Clin Exp Ophthalmol. 2022; doi:10.1007/s00417-022-05794-4. 77. Xiong R, Zhu Z, Jiang Y, et al. Longitudinal changes and predictive value of choroidal thickness for myopia control following repeated low-level red-light therapy. Ophthalmology. 2022; doi:10.1016/j.ophtha.2022.10.002. 78. Yang W, Lin F, Li M, et al. Immediate effect in retina and choroid after 650 nm low-level red light therapy in children. Ophthalmic Res. 2022; doi:10.1159/000527787. 79. Xiong R, Zhu Z, Jiang Y, et al. Sustained and rebound effect of repeated low-level red-light therapy on myopia control: A 2-year post-trial follow-up study. Clin Exp Ophthalmol. 2022;50(9):1013-24. 80. Thakur S, Dhakal R, Verkicharla PK. Short-term exposure to blue light shows an inhibitory effect on axial elongation in human eyes independent of defocus. Invest Ophthalmol Vis Sci. 2021;62(15):22. 81. Flitcroft DI. The complex interactions of retinal, optical and environmental factors in myopia aetiology. Prog Retin Eye Res. 2012;31(6):622-60. 82. Flitcroft DI, Harb EN, Wildsoet CF. The spatial frequency content of urban and indoor environments as a potential risk factor for myopia development. Invest Ophthalmol Vis Sci. 2020;61(11):42. 83. Wu PC, Tsai CL, Wu HL, et al. Outdoor activity during class recess reduces myopia onset and progression in school children. Ophthalmology. 2013;120(5):1080-5. 84. He M, Xiang F, Zeng Y, et al. Effect of time spent outdoors at school on the development of myopia among children in China a randomized clinical trial. JAMA. 2015;314(11):1142-8. 85. Wu PC, Chen CT, Lin KK, et al. Myopia prevention and outdoor light intensity in a school-based cluster randomized trial. Ophthalmology. 2018;125(8):1239-50. 86. Jin JX, Hua WJ, Jiang X, et al. Effect of outdoor activity on myopia onset and progression in school-aged children in northeast China: The Sujiatun eye care study. BMC Ophthalmol. 2015;15(1):1-11. 87. Fujiwara M, Hasebe S, Nakanishi R, et al. Seasonal variation in myopia progression and axial elongation: an evaluation of Japanese children participating in a myopia control trial. Jpn J Ophthalmol. 2012;56(4):401-6. 88. Gwiazda J, Deng L, Manny R, et al. Seasonal variations in the progression of myopia in children enrolled in the correction of myopia evaluation trial. Invest Ophthalmol Vis Sci. 2014;55(2):752. 89. Parssinen O, Lyyra AL. Myopia and myopic progression among schoolchildren: A three-year follow- up study. Invest Ophthalmol Vis Sci. 1993;34(9):2794-2802. 90. Sánchez-Tocino H, Villanueva Gómez A, Gordon Bolaños C, et al. The effect of light and outdoor activity in natural lighting on the progression of myopia in children. J Fr Ophtalmol. 2019;42(1):2-10. 91. Zhang M, Li L, Chen L, et al. Population density and refractive error among Chinese children. Invest Ophthalmol Vis Sci. 2010;51(10):4969-76. 92. Lu B, Congdon N, Liu X, et al. Associations between near work, outdoor activity, and myopia among adolescent students in rural China: The Xichang Pediatric Refractive Error Study report no. 2. Arch Ophthalmol. 2009;127(6):769-75. 93. Jonas JB, Ang M, Cho P, et al. IMI prevention of myopia and its progression. Invest Ophthalmol Vis Sci. 2021;62(5):8-10. |